
Congress Waking up to 340B Corporate Slush Fund
This op-ed was written by Ellen Weaver and Lindsay Boyd and published in The Hill on 5/26/15.
By the time it got to the president’s desk, the final page tally of the Affordable Care Act came in at 2,700 pages. As Rep. Nancy Pelosi (D-Calif.) so famously said, we had to “pass it to know what’s in it,” so it’s little wonder that unpleasant surprises have awaited us around every corner.
For proof, consider the rapid expansion of the federal 340B drug program – the latest in a long string of provisions buried in those thousands of pages that are finally seeing the light of day.
The 340B program, created by Congress over two decades ago, was originally intended to help vulnerable and uninsured patients gain access to prescription medicines. Since then, the program has ballooned to a multi-billion dollar slush fund for hospitals—on the backs of low-income patients—thanks to minimal government oversight and new expansions authorized within Obamacare.
The way it works is fairly simple. The federal government requires pharmaceutical manufacturers to provide steep discounts to hospitals that qualify for 340B. Yet, many hospitals don’t always pass along the discounts to the low-income patients they are meant for and instead, turn around and charge patients full price for these drugs—all the while pocketing the additional profits. Some chain pharmacies have even gotten in on the act by contracting to be extensions of the hospital pharmacy.
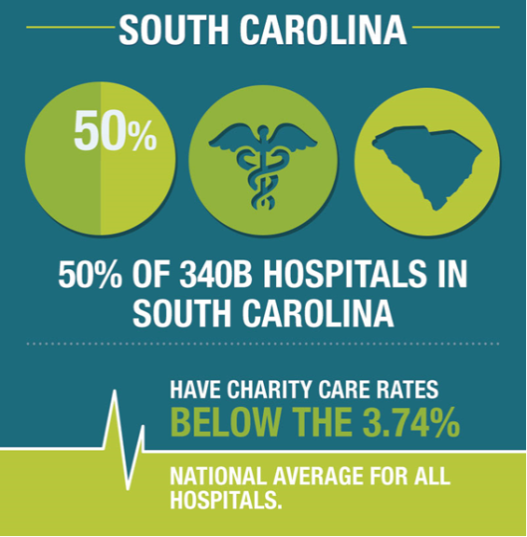
Now, a program that was originally created to serve 90 truly safety-net hospitals is serving more than 10,000. Spending on the program has skyrocketed from $1.1 billion in 1997 to more than $7 billion in 2013, and that number is projected to hit $16 billion by 2020. It’s also worth noting that the national average for charity care in hospitals is 3.3 percent of their total patient care. In Tennessee 67 percent of 340B hospitals and in South Carolina 50 percent of 340B hospitals provide less charity care than the national average.
At the state level, these numbers should be particularly riveting for lawmakers who have been pummeled by hospitals to support Medicaid expansion under the guise of “operating on razor-thin margins.” In Tennessee, Governor Haslam (R) told taxpayers that hospitals could be trusted not to shift costs to patients when they agreed to help finance his expansion proposal. If their 340B actions are any indication of whether they can be trusted, Tennesseans should be greatly alarmed. And in South Carolina, while hospitals in many rural areas struggle, cost data filed with the federal government shows that taken together, Palmetto State hospitals made $1.1 billion in profits in 2013 – a 70 percent increase over 2011.
Thankfully, Congress is beginning to ask important oversight questions, including the obvious: what are hospitals and pharmacies doing with all of the money now flowing from the 340B program?
The U.S. House Energy & Commerce Subcommittee on Health was troubled by these revelations and recently held a hearing on the topic. Chairman Joe Pitts (R-Pa.) led the investigation and Tennessee Rep. Marsha Blackburn (R) asked tough questions about the rapid growth of the program, the need for accountability, the statutory definition of “patient” and the process for distributing 340B funds. Sen. Chuck Grassley (R-Iowa) has also been a sharp critic of the program—including his questioning of Duke University’s $463 million generated in just four years through 340B.
So far, what they’ve gotten are hazy answers, at best. Details have proved scarce and at the end of the day, hospitals profiting from this arrangement seem to be saying, “Trust us, we’re spending the money on the poor.”
Sen. Lamar Alexander (R-Tenn.), chairman of the Senate HELP Committee with jurisdiction over 340B, has gone on record calling for 340B reform. And South Carolina Sen. Tim Scott (R) is now an important member of that committee. With their leadership, the Senate should demand a hearing on 340B and compel action to guarantee that 340B discounts flow back to the most vulnerable or uninsured patients directly, instead of padding administrative bottom lines.
Patients and taxpayers in our states are at the mercy of Congressional action to rein in abuse of 340B and restore the program’s original intent. Despite Congress’ long to-do list, this is one that should be a no-brainer. The time to act is now.
Weaver is the president and CEO of the Palmetto Promise Institute in South Carolina and Boyd is the director of Policy at The Beacon Center of Tennessee.