Direct Primary Care: “Innovating Backwards”
What is Direct Primary Care?
According to Dr. Jerome Aya-ay, a family-medicine physician with offices in Greenville, Spartanburg and Columbia, Direct Primary Care (DPC) is very simple: “It is a relationship between a patient and their physician.”
For a flat, monthly fee (often called membership dues), patients receive preventative and diagnostic medical care. Unlike some “concierge care” models, where high monthly fees and insurance companies are billed for service, Direct Primary Care practices rely solely on membership dues paid by the patient or fees for a la carte services.
According to a recent Forbes article, doctors are able to cut 40% of their operating budget by eliminating the administrative costs associated with billing insurance companies for services provided.[1] At Palmetto Proactive Healthcare, a Direct Primary Care clinic operating in South Carolina, an estimated $90,000 per physician per year cost savings results in a $60 per month membership fee for individual patients — that’s less than an average monthly cell phone bill!
The simplicity of the model might sound too good to be true.However, by jettisoning insurance contracts, third party payers and red-tape, Direct Primary Care physicians are “innovating backwards” — marketing their services at an affordable rate, competing with other DPC practices to keep prices low and re-establishing the principle that healthcare should be about maintaining relationships and trust, not navigating complicated and expensive systems.
Why Direct Primary Care?
South Carolina’s backbone is the middle class. According to the US Census Bureau, 44.4% of South Carolinians make between $25,000 and $75,000 per year, and 72% of South Carolinians make less than $100,000 per year.[2] For these middle-income earners, the rising cost of healthcare, coupled with the sheer expense of having and using insurance — especially now that South Carolina is down to one Obamacare insurance provider — leaves citizens with hard decisions about prioritizing expenses.
Direct Primary Care offers these South Carolinians access to cheaper drugs, all the preventative care they need, blood work and round the clock access to a physician without having an insurance company involved. Adequate preventative care and savings earned by access to cheaper drugs might enable families to afford catastrophic insurance coverage, returning insurance to its primary purpose of covering unforeseen risk. No one uses their car insurance for routine maintenance — it should be the same with health insurance.
Direct Primary Care in South Carolina
Direct Primary Care practices are not currently illegal in South Carolina, but they are under threat. Effective lobbying funded by large insurance companies and ever-increasing regulations threatens the ability of innovative, risk-taking physicians to make primary care available and affordable. So what can states like South Carolina do to make sure Direct Primary Care practices remain available to the people of South Carolina?
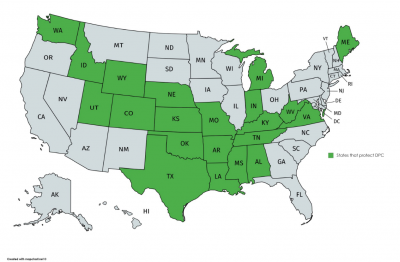
- Define DPC outside the insurance code. 23 states around the country have taken this route to protect DPC from being labeled as a “risk-bearing entity,” which would subject DPC practices to a whole host of new regulations intended to govern insurance companies.
- Resist calls to limit benefits. South Carolina must not regulate DPC under the Department of Insurance, institute patient caps or centrally define what services can be provided at DPC practices. Limitations like these only make access to more affordable healthcare harder to find and directly contradict free-market principles.
- Understand the limits of Direct Primary Care and the problem it has diagnosed and is trying to solve. A once-a-month membership fee to a primary care doctor does not fulfill the insurance mandate under Obamacare. With the exception of a few practices (such as the Surgery Center of Oklahoma), Direct Care outside of family medicine is rare. Patients still need “wraparound” or “catastrophic” coverage to see specialists. Direct Primary Care is not insurance and is not intended to replace it. Instead it is intended to be a supplement to the healthcare market, giving patients access to more affordable, quality choices in an ever-more complicated and costly environment.
Additional Benefits of Direct Primary Care
Direct Primary Care places a spotlight on what exactly the free-market is capable of providing in the healthcare industry, but there are two other reasons to protect DPC:
- A la carte care: For some South Carolinians, signing up for a monthly membership is not desirable. What these patients really want might just be a quick check-up or a one-time service. Direct Primary Care medical clinics offer competitively priced a la carte services. Though taking advantage of more than one a la carte service will quickly add up to a monthly membership fee or more, DPC centers know it should be the patient’s choice.
- Transparency in Pricing: One reason DPC works is transparency in pricing. At a DPC clinic, patients know how much they are paying and what services are associated with the cost, as opposed to being surprised by outrageous bills that come weeks after care. On this issue DPC is meeting growing patient demand. Some hospitals have begun informing patients up front about the costs associated with care. Other legislative bills like Right to Shop are making their way through state legislatures right now, but DPC is ahead of the curve in empowering patients to be shoppers.
The Future of Direct Primary Care
Dr. Keith Smith, a specialist at the Surgery Center of Oklahoma, is demonstrating what the future of Direct Care might look like. One glance at the “pricing” section on their website and you’ll see the specialized types of surgery they offer and the bottom line price you’ll pay.[3]
Of course, surgery is more expensive than a yearly check-up, but the model is the same and the Surgery Center of Oklahoma is blazing the trail. For example. Art Villa, an outdoorsman from Montana, paid $19,000 for his entire knee replacement surgery at the Surgery Centy of Oklahoma. If he had gone to his local hospital, the surgery itself would have cost him $40,000, and that does not include anesthesiologist’s fees and a host of other cost extras.[4]
In South Carolina, paving the way for Direct Care means moving immediately to protect Direct Primary Care as an option for Palmetto State patients.
States that Protect Direct Primary Care